
Despite impressive progress in reducing racial disparities in health and well-being, black Americans are still among the least healthy groups in the United States. This is particularly true for black children, who fare poorly on a host of health outcomes, including everything from asthma incidence to infant and child mortality. However, some black children fare much better than others. In a recent paper published in the American Journal of Public Health, my co-authors and I examine how health among black children varies by the child’s and mother’s birthplace. We find that black children with foreign-born mothers are substantially healthier than those with U.S.-born mothers, and that this advantage further varies by mother’s region of birth.
We considered five health outcomes: general health status, the number of school days missed in the last year due to illness, whether the child was diagnosed with an allergy in the last 12 months, whether the child has ever been diagnosed with asthma, and whether the child has any physical activity or cognitive limitations. Using data from the 2000-2011 National Health Interview Surveys, we analyzed how each of these five health outcomes differed by mother’s global region of birth and by whether the child was U.S.-born. Since the great majority of American blacks born abroad immigrated from either Africa or Latin America and the Caribbean, we restrict attention to children whose mothers were born in these regions and in the U.S.
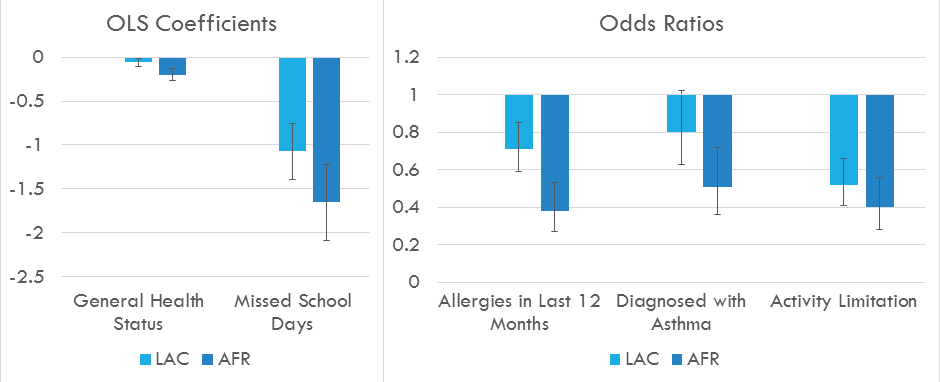
Source: Hendi, Mehta, and Elo (2015)
As shown in Figure 1, children whose mothers were born in Africa had the most favorable health profiles, followed by those whose mothers were born in Latin America and the Caribbean, with children of U.S.-born mothers having the worst outcomes. We find that differences in mother’s education, family income, and mother’s marital status do not entirely explain these differences. What’s perhaps more surprising is that even among children with foreign-born mothers, children who were born abroad do better on objective health measures than children born in the U.S.
What might explain these findings? One possibility is that the mothers who emigrated from Africa are healthier than those from Latin America and the Caribbean. If health is partly heritable—and prior evidence suggests that it is—then we would expect part of the health gradient to be due to variation in the mothers’ health profiles. However, we found that adjusting for mothers’ health and smoking status did not explain the child health gradient. Another possibility is that the child health gradient is due to differences across origin groups in the recency of migration. The hypothesis is that either more recent immigration cohorts have some unobserved capacity for better child health, or that longer family exposure to the United States is detrimental for the child’s health. The latter could be because families pick up health behaviors or live in environments that do not support good health. We adjusted our statistical models for recency of migration and find that mother’s time in the U.S. does indeed explain a large part (though not all) of the difference in health levels between children with mothers from Latin America and the Caribbean versus Africa.
Why is it important to understand how patterns of migration play a role in determining the health of black children? The answer is: for many reasons! First off, understanding the determinants of and improving child health are desirable and necessary goals in their own right. Understanding why children of black immigrants have better health than black children with U.S.-born mothers helps us answer the question, “What about our society leads to black children having such poor health outcomes?” Second, as immigration continues to shape the makeup of our nation, more and more blacks will be children of immigrants. A little-appreciated fact is that today, around 20% of black children are the children of immigrants, and this proportion is expected to keep growing in the coming years. In order to track progress in reducing disparities in child health and to understand potential future challenges, it’s important to know more about black immigrant families. Third, as the population ages, children of immigrants will make up a larger share of the adult population. Almost all immigrant-origin groups have lower mortality and better health than the U.S.-origin population, and we have every reason to believe this will be the case for blacks whose parents immigrated to the U.S. All else being equal, we can expect to see dramatic future improvements in levels of mortality and health among black adults due in part to the increasing presence of children of immigrants.
You must be logged in to post a comment.